73 வயது ஐயா
இவருக்கு சர்க்கரை இல்லை.
வலது கால் பாதத்தில் ஒரு வாரத்திற்கு முன்பு ஒரு சிறிய காயம் ஏற்பட்டுள்ளது.
வலது காலில் வீக்கம் ஏற்பட்டு காய்ச்சலுடன் எங்கள் மருத்துவமனைக்கு அழைத்து வந்தார்கள்.
அவருக்கு அதிகமான காய்ச்சலும்(38.9`C) இருதயத்துடிப்பும் அதிகமாக இருந்தது.
கால் வீக்கம் அதிகமாக இருந்தது.
கால் முழுவதும் சிறிய நீர்க்கட்டிகள் (blisters) இருந்தன.
அவரது ரத்தப் பரிசோதனை முடிவுகள்.
Blood Sugar: 130 mg/dL
Blood Urea: 32 mg/dL
Serum Creatinine: 1.2 mg/dL
Total WBC Count: 25,300 cells/cumm
Hemoglobin: 11.2 g/dL
அவருக்கு இருந்த நோய்….
*Necrotizing fasciitis of the right leg and foot
*Septicemia
சலம் கால் முழுவதும் பரவி இரத்தத்திலும் கலந்து இருந்தது.
இதனால் இரத்தத்தில் வெள்ளை அணுக்களின் எண்ணிக்கை அதிகமாக இருந்தது.
அட்மிஷன் செய்து அவருக்கு முறையான Antibiotics மருந்துகள் கொடுத்தோம்.
4வது நாள் அவரது காய்ச்சல் குணமானது.
ஆனால் கால் வீக்கம் அதிகமாய் இருந்தது.
5வது நாள் அவரது காலில் ஒரு அறுவை சிகிச்சை செய்து காலில் பாதிக்கப்பட்ட பகுதிகள் மற்றும் நீரை வெளியேற்றினோம்.
அதற்குப் பின் அவரது இரத்த அளவு (Hb) குறைந்ததால் அவருக்கு ரத்தம் செலுத்தப்பட்டது.
பத்து நாட்களில் அவரது கால் வீக்கம் குறைய ஆரம்பித்து விட்டது.
15 வது நாள் அவரை வீட்டிற்கு அனுப்பி வைத்தோம்.
தினமும் வந்து கால் புண்ணை சுத்தம் செய்து ட்ரெஸ்ஸிங் போட்டுக் கொண்டார்.
30 நாட்களில் மீண்டும் ஒருமுறை அவரை அட்மிஷன் செய்து பாதிக்கப்பட்ட பகுதிகள் சிலவற்றை நீக்கினோம்.
ஆறு வாரங்களில் அவரது புண் நன்றாக குணமாகியது.
ஆனால் பெரிய புண்ணாக இருப்பதால் ஆறுவதற்கு தாமதம் ஆகும் என்பதால் தோல் ஒட்டும் அறுவை சிகிச்சை செய்ய முடிவு செய்தோம்.
அதன்படி தோல் ஒட்டும் அறுவை சிகிச்சை செய்யப்பட்டு 15 நாட்களில் புண் முழுவதுமாக ஆறிவிட்டது.
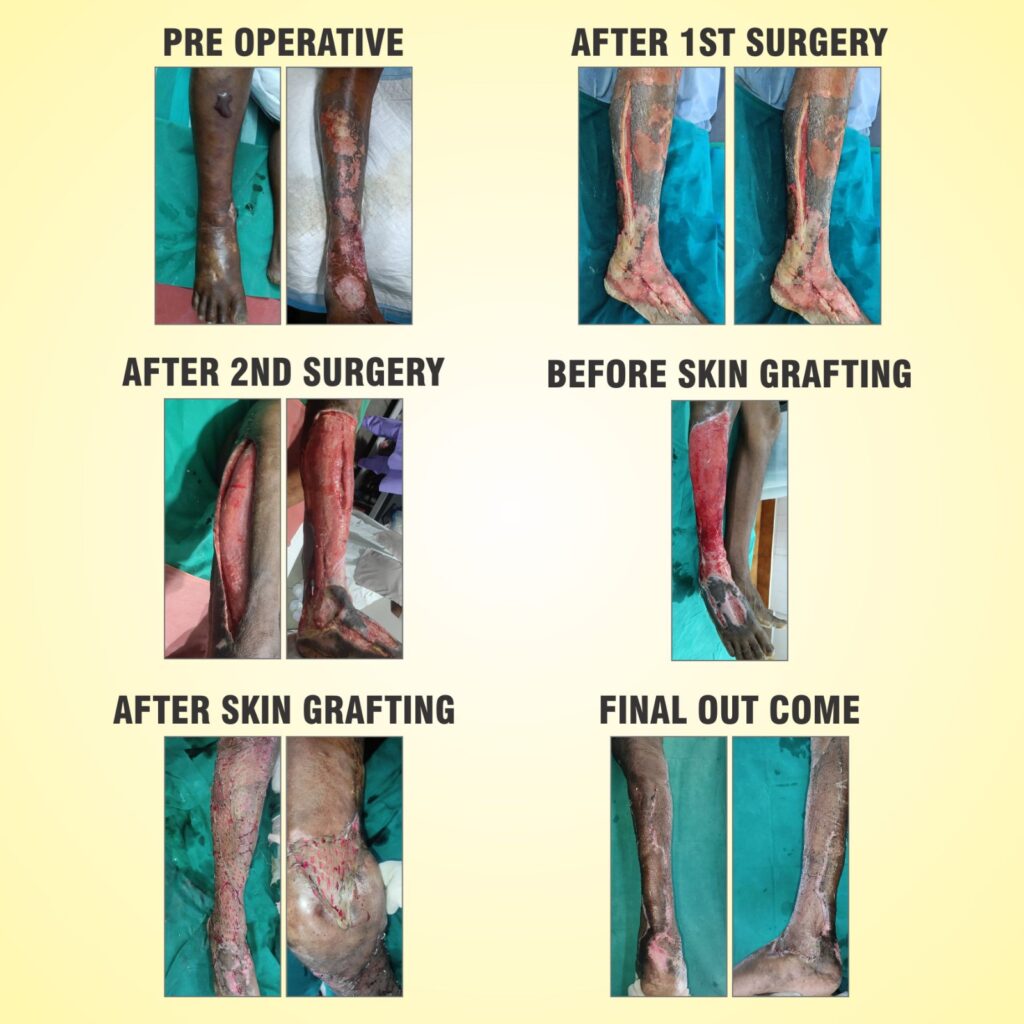
மிகப்பெரிய ஆபத்திலிருந்து மீண்டு வந்த அந்த 73 வயது ஐயா, தற்போது நலமுடன் வாழ்ந்து வருகிறார்.
அதற்கான படங்களை பதிவிட்டுள்ளோம்.
A 73-year-old male patient came to our hospital with:
Painful swelling in the right leg and foot since the previous night
On and off fever
H/O Injury Rt leg (+) 1 week before
Clinical Examination
Patient was conscious and oriented
Had fever (38.9`C) and increased heart rate (tachycardia)
Local Examination (Right Leg):
Multiple blisters over the foot and lower part of the leg
Tenderness (+)
Signs of inflammation (+)
Pus discharge (+)
Investigations
Blood Sugar: 130 mg/dL
Blood Urea: 32 mg/dL
Serum Creatinine: 1.2 mg/dL
Total WBC Count: 25,300 cells/cumm
Hemoglobin: 11.2 g/dL
Diagnosis
*Necrotizing fasciitis of the right leg and foot
*Septicemia
Treatment Given
Patient was admitted and started on broad-spectrum antibiotics and Metronidazole.
After stabilization (on 5th day), wound debridement surgery was done by our plastic surgeon
Post-Operative Course
Hemoglobin dropped to 7 g/dL → Patient received blood transfusion (whole blood + FFP)
Swelling gradually reduced by the 10th post-operative day
Patient showed good recovery
Discharged on the 15 th day of admission
Follow-Up Care
Wound debridement 2nd time 30 th day of previous admission
Regular wound cleaning and dressing in OPD
Healthy granulation tissue formed in 6 weeks
Wound not fully covered → planned for skin grafting
Skin grafting done under spinal anesthesia by our plastic surgeon
Donor and recipient sites healed well within 15 days of skin grafting
Final Outcome
Blood tests returned to normal
Hemoglobin improved to 10 g/dL
Overall recovery was successful
#NECROTIZING FASCITIS
Necrotizing fasciitis is a severe, rapidly progressive soft tissue infection commonly seen in mixed infections such as diabetic foot. It begins with a trivial infection, but due to thrombotic occlusion of small blood vessels, tissue necrosis develops. Normally, after infection control, arterioles recanalize and healing occurs through granulation tissue formation; however, in necrotizing fasciitis, virulent organisms like staphylococci and streptococci release angiotoxic substances such as alpha-toxin, along with spreading factors like streptokinase and hyaluronidase. These toxins destroy fibrin barriers and connective tissue, allowing the infection to spread rapidly along fascial planes, leading to necrosis of subcutaneous tissues up to the muscle fascia. Clinically, it presents with rapidly worsening pain, erythema, swelling, dusky skin discoloration, and hemorrhagic blisters. The vascular occlusion worsens progressively, converting small lesions into extensive areas of necrosis and gangrene within a short period. Systemic toxicity with fever, tachycardia, and hypotension is common, indicating sepsis. Immediate management with aggressive surgical intervention such as fasciotomy, fasciectomy, or even amputation, along with intensive medical treatment, is essential to prevent a life-threatening outcome.
References:
DIABETIC FOOT:
A Clinical Atlas / Sharad Pendsey